

A workplace drug-diversion investigation is the structured inquiry into the theft or misuse of controlled substances by employees—most often in hospitals, clinics, and pharmaceutical operations. It combines automated dispensing-cabinet analytics, discrepancy and waste reconciliation, and forensic review to identify a diverter, then preserves defensible evidence for DEA reporting, state-board action, criminal referral, and termination—while protecting patient safety and the organization’s controlled-substance license.
Drug diversion is unlike almost any other workplace investigation, because a misstep does not merely lose a case—it can leave a patient exposed to a saline-substituted syringe, a nurse continuing to practice impaired, and an organization out of compliance with the Controlled Substances Act. The stakes are simultaneously clinical, criminal, regulatory, and reputational. This guide sets out how an elite investigations team detects diversion, converts data anomalies into admissible evidence, navigates DEA and state-board obligations, and remediates the control failure that allowed it—across both clinical and industrial environments.
What Is Drug Diversion, and Where Does It Happen?
Drug diversion is the transfer of a controlled substance from its lawful medical or commercial purpose to an illicit one. In practice that means an employee stealing narcotics, sedatives, or stimulants—for personal use, for sale, or both. It is a crime, a patient-safety threat, and a breach of a regulated institution’s duty as a Drug Enforcement Administration registrant.
The environments differ, but the exposure is constant:
- Acute-care hospitals—the highest-volume setting, where anesthesia, surgical, emergency, and critical-care units handle large quantities of opioids and the diverter is frequently a licensed clinician with legitimate access.
- Ambulatory surgery centers, clinics, and dental and veterinary practices—smaller teams and thinner oversight, where a single trusted employee may control ordering, stocking, and reconciliation.
- Long-term care and hospice—end-of-life opioid regimens and after-death drug destruction create documentation gaps that are readily exploited.
- Retail and hospital pharmacies—inventory-level theft from bulk stock, altered dispensing records, and forged prescriptions.
- Industrial and commercial settings—pharmaceutical manufacturers, wholesale distributors, third-party logistics, and research laboratories, where diversion looks less like a nurse pocketing a vial and more like inventory shrinkage, falsified destruction records, and warehouse or supply-chain theft governed by the same CSA security requirements.
The common thread is trusted internal access. Diversion is an insider problem, and—like the broader discipline of the internal investigation—it demands methods that assume the subject knows the systems, controls some of the evidence, and will act to conceal once alerted.
How Is Drug Diversion Detected?
Most diversion surfaces not through a confession or a witness, but through data. Modern controlled-substance workflows generate a dense audit trail—every withdrawal, override, waste, and count is timestamped and attributed to a user. Diversion is the deviation from the expected pattern, and detection is the disciplined analysis of that deviation. The signals below are the ones a competent investigation isolates first.
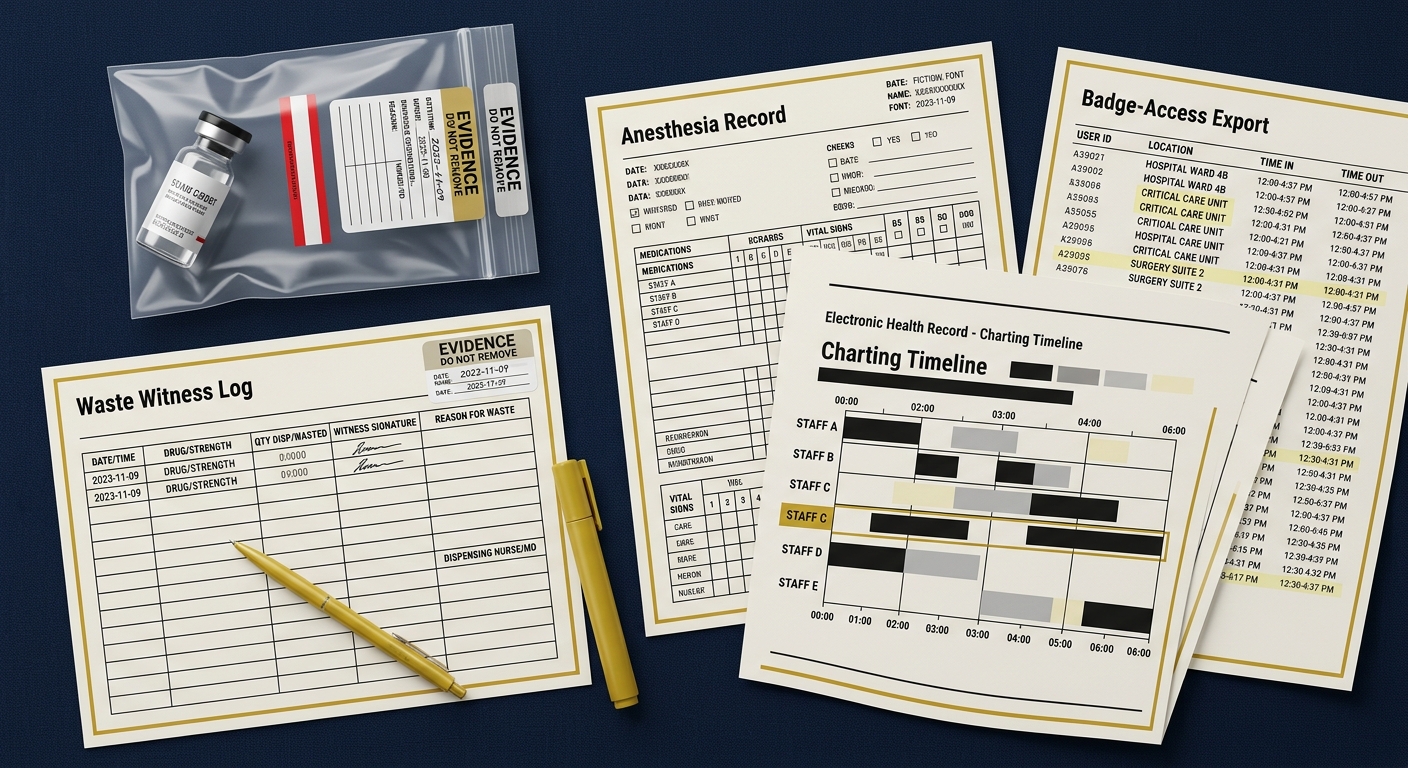
| Data stream | Red-flag pattern | What it may indicate |
|---|---|---|
| Automated dispensing cabinets (Pyxis, Omnicell) | Override rates and withdrawal volume far above unit and peer baselines; repeated cancelled or discrepant transactions | Removing controlled substances outside the patient profile to pocket them |
| Waste documentation | Missing, late, or unwitnessed waste; waste consistently clustered at shift end | Diverting the portion recorded as “wasted” |
| Anesthesia and procedural records | Mismatch between drug drawn, administered, and charted; heavy reliance on a single provider’s undocumented “waste” | Substituting saline or under-documenting to skim the balance |
| Dispense-to-charting timing | Long or irregular gaps between cabinet removal and administration charting | Removing drug early to divert before documenting |
| Patient records / MAR | Controlled meds pulled for discharged, transferred, or non-existent patients, or without an order | “Ghost patient” diversion |
| Perpetual inventory (pharmacy / warehouse) | Recurring count discrepancies isolated to one unit, shift, or employee | Bulk theft from stock or falsified destruction |
The critical analytic principle is peer comparison. A single override proves nothing; a clinician whose override, waste, and per-patient consumption sit several standard deviations above every peer on the same unit, shift after shift, is a pattern. Dedicated diversion-analytics platforms now automate much of this surveillance, but software raises a flag—it does not build a case. What separates a defensible investigation from a wrongful-termination lawsuit is what happens after the flag: the transaction data must be preserved, corroborated, and interpreted by someone who understands both clinical workflow and evidentiary standards.
What Are the Regulatory and DEA Obligations?
Diversion sits inside a dense regulatory frame, and an organization’s response is itself a compliance obligation. Handling a suspected loss quietly and internally, without meeting reporting duties, can compound a single employee’s theft into an institutional violation.
- The Controlled Substances Act and DEA registration. Any facility that stores or dispenses controlled substances is a DEA registrant bound by the security and recordkeeping requirements of 21 CFR Part 1301, including an affirmative duty to guard against theft and diversion. Guidance and forms are published by the DEA Diversion Control Division.
- DEA Form 106. A registrant must report the theft or significant loss of controlled substances to the DEA, in writing, upon discovery—documenting the substances, quantities, and circumstances. Determining whether a loss is “significant,” and when the clock starts, is a judgment call best made with counsel.
- State licensing boards. Boards of nursing, pharmacy, and medicine typically require reporting of an impaired or diverting licensee, and many operate confidential alternative-to-discipline monitoring programs. A parallel report to the relevant board usually runs alongside the DEA filing.
- Accreditation and payer standards. Medication-management and controlled-substance standards from bodies such as The Joint Commission, along with the Centers for Medicare & Medicaid Services Conditions of Participation, expect an active diversion-prevention and response program—not merely a reaction after the fact.
- Patient-safety and notification duties. Where diversion involved tampering—refilling used syringes, substituting saline—patients may have been exposed to infection, triggering public-health notification obligations. Injection-safety and diversion resources from the Centers for Disease Control and Prevention inform that assessment.
Because these duties run in parallel and on their own timelines, the reporting strategy is decided early and documented—not improvised once the investigation is already public.
The Eight-Phase Diversion Investigation Framework
An elite diversion investigation follows a fixed sequence built to protect patients, preserve evidence, and satisfy every regulator that reviews the file afterward. The order is not cosmetic—building the data case before the subject is alerted is what makes the outcome defensible.
- Trigger and triage. A flag arrives—an analytics alert, a colleague’s report, an unexplained shortage, or a patient’s inadequate pain relief. Capture it verbatim, assess immediate patient-safety risk, and decide whether interim measures (reassignment away from controlled-substance access, heightened witnessing) are warranted without prejudging.
- Assemble the team and settle privilege. Diversion is multidisciplinary—pharmacy, nursing leadership, risk, security, and counsel. Structure the inquiry under attorney direction where litigation or regulatory exposure is real, so work product is protected and investigators act as counsel’s agents.
- Preserve the data forensically. Export and hash dispensing-cabinet logs, medication administration records, anesthesia records, badge/access data, and inventory records before the subject knows, because live systems purge, roll over, and can be edited. This is where digital forensics discipline begins.
- Build the diversion timeline. Reconcile what was removed against what was administered, charted, wasted, and returned—mapped per patient, per shift, per employee. Peer-compare against colleagues doing the same work. The output is an objective, records-based timeline, not an accusation from memory.
- Corroborate beyond the data. Layer in physical evidence (tamper-evident packaging, recovered vials, sharps), access and camera records, financial indicators where relevant, and, where tampering is suspected, laboratory drug testing of suspect vials. This physical and financial corroboration is what elevates a statistical pattern into proof.
- Interview outward-in. Witnesses and supervisors first, the subject last, so the subject responds to specific, evidenced findings rather than a fishing expedition.
- Findings and mandated reporting. Reach findings on a preponderance standard, then execute the reporting strategy—DEA Form 106, state-board notification, and any patient-safety disclosures—on their required timelines.
- Remediate and harden. Address the individual, then close the control gap the case exposed so the same failure cannot recur.
Why Does Chain of Custody Decide These Cases?
Diversion cases are won or lost on evidentiary integrity. The proof is a mix of digital records and physical items—vials, syringes, packaging, and, sometimes, the substituted fluid inside them—and each category must be handled so that its authenticity cannot be attacked later by defense counsel, an arbitrator, or a licensing board.
On the digital side, dispensing-cabinet exports, medication records, and access logs are collected in a forensically sound manner, hashed, and documented so that the dataset presented months later is provably identical to what the system held on the day of collection. On the physical side, every recovered vial or syringe is labeled, sealed in tamper-evident packaging, logged, and tracked through a documented custody chain from recovery to laboratory analysis—because a suspect vial that tested as saline is only persuasive if its handling is unbroken. A single unlogged transfer, an edited spreadsheet, or a vial left in an unsecured drawer is enough to reduce a compelling data pattern to inadmissible noise. The same rigor that governs a courtroom exhibit is described in our guidance on forensic evidence handling, and it applies with equal force here.
How Are Diversion Interviews Conducted?
By the time the subject is interviewed, the investigator already knows the timeline. The interview tests the subject’s account against the record; it is not a search for a theory. Diversion interviews carry unique sensitivities because the subject is frequently a respected clinician, addiction is often the driver, and the conversation may implicate both criminal exposure and a professional license.
- Interview witnesses and supervisors first. Establish workflow norms—how waste is witnessed on this unit, what overrides are routine—so the subject’s deviations stand out against an established baseline rather than a hypothetical one.
- Prepare from the evidence. Enter with the reconciled timeline and the specific transactions to be addressed. Never interview blind.
- Use a two-person team. A dedicated notetaker preserves an accurate record and provides corroboration if the account is later disputed.
- Stay neutral and non-accusatory. Present discrepancies and invite explanation. Impairment and diversion frequently coexist; a coercive interview can taint the record and endanger a person who may need medical intervention.
- Do not practice medicine or law. Investigators document conduct; they do not diagnose addiction or render criminal conclusions. Findings speak to policy and evidence, and refer the clinical and legal determinations to the proper authorities.
- Give a genuine hearing. Record the subject’s response fully. A rushed, one-sided interview is the foundation of a later “sham investigation” or wrongful-termination claim.
What Does Remediation Look Like After a Diversion Case?
Identifying the diverter closes only half the matter. The other half is fixing the environment that permitted diversion to go undetected—often for far longer than leadership assumes. Remediation runs on two tracks.
- The individual. Proportionate, consistently applied action—termination, referral to law enforcement, and mandatory board reporting, coordinated so that criminal, regulatory, and employment tracks do not undercut one another. Where a monitoring or alternative-to-discipline program applies, it is engaged through the appropriate board.
- The system. Close the control gap the case exposed: tighten witnessed-waste procedures, reduce blanket override privileges, deploy or tune diversion-analytics surveillance, reconcile anesthesia records routinely, secure return and destruction workflows, and align policy with CSA security requirements. A single detected diverter almost always signals a monitoring blind spot rather than a lone anomaly.
The organizations that recover best treat a diversion event as a diagnostic on their entire controlled-substance program—a discipline that overlaps closely with proactive healthcare and hospital security, where physical safeguards, access control, and surveillance are engineered before an incident rather than after it.
What Distinguishes an Elite Diversion Investigation?
The difference between a defensible investigation and a costly one is rarely effort—it is method. The recurring failures are predictable:
- Confronting the subject before preserving the data—the fastest route to purged logs and coordinated stories.
- Treating an analytics flag as a finding—acting on software output without corroboration, then losing the wrongful-termination suit.
- Breaking chain of custody—an unsealed vial or an edited export that turns proof into inadmissible noise.
- Missing reporting obligations—handling it “internally” and converting one employee’s theft into an institutional CSA violation.
- Ignoring patient safety—failing to assess tampering-related infection risk and notification duties.
- Fixing the person, not the system—terminating the diverter while leaving the blind spot open for the next one.
National Reach, Discreet Command
Honeybadger Solutions conducts controlled-substance diversion investigations for healthcare systems, surgical centers, pharmacies, and pharmaceutical operations across Arizona, nationwide, and internationally. Our digital forensics, financial investigations, and background-intelligence functions are in-house and remote-by-design, so dispensing-cabinet and records preservation can begin within hours of a trigger, wherever the facility is located. Field, physical-security, and protective operations are commanded through a vetted-partner network, with Arizona as home command and established theaters in California, Texas, and Florida. Whether the matter is a single suspected clinician or an enterprise-wide inventory loss, the standard does not change—explore our full corporate investigations, healthcare security, and security capabilities.
Frequently Asked Questions
How is drug diversion first detected in a hospital? Most often through data rather than a witness. Automated dispensing-cabinet analytics flag a clinician whose withdrawals, overrides, waste, or per-patient consumption run far above peers on the same unit and shift. Discrepancy reports, unwitnessed waste, charting gaps, and patient reports of inadequate pain relief are common corroborating signals. A flag is a starting point, not proof—it must be preserved and corroborated before any action.
Does an employer have to report drug diversion to the DEA? Generally yes. A DEA registrant must report the theft or significant loss of controlled substances on DEA Form 106 upon discovery, and most state nursing, pharmacy, and medical boards require reporting of an impaired or diverting licensee. Because these duties run in parallel on their own timelines, the reporting strategy should be set early, with counsel, rather than after the investigation becomes public.
Why is chain of custody so important in diversion cases? Because the evidence is a mix of digital records and physical items—vials, syringes, and packaging—that will be scrutinized by defense counsel, arbitrators, and licensing boards. Digital exports must be collected forensically and hashed; physical items must be sealed, labeled, logged, and tracked to the lab. A single unlogged transfer or edited file can render an otherwise compelling case inadmissible.
Does drug diversion occur outside hospitals? Yes. It occurs in clinics, dental and veterinary practices, long-term care, hospice, and retail and hospital pharmacies, and in industrial settings such as pharmaceutical manufacturers, wholesale distributors, logistics providers, and research laboratories. In those environments diversion looks more like inventory shrinkage, falsified destruction records, and supply-chain theft—governed by the same Controlled Substances Act security requirements.
About Honeybadger Solutions
Honeybadger Solutions is an Arizona-licensed security and investigations firm serving all of Arizona, the nation, and international clients. We combine in-house digital forensics, cybersecurity, financial investigations, and background intelligence with a vetted network for field, physical-security, and protective operations. Our teams run discreet, defensible controlled-substance diversion investigations built to protect patients, satisfy DEA and state-board scrutiny, and withstand litigation and arbitration.
Three offices: Casa Grande (HQ), Phoenix, and Oro Valley. To discuss a confidential matter, call 602-725-2818. Learn more about our corporate and internal investigations capabilities and request a discreet consultation.